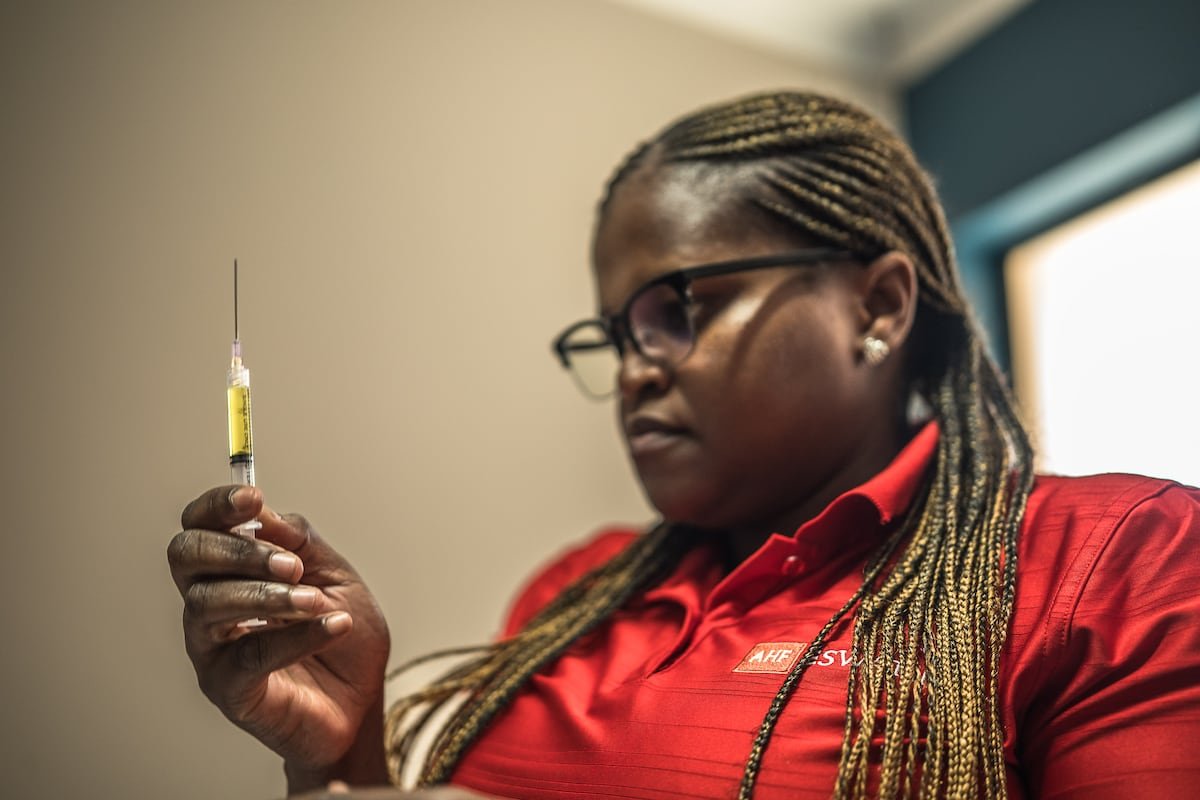
Precious closes her eyes and clenches her fists as the syringe needle penetrates her right thigh, slowly injecting a greenish-yellow liquid. The same procedure is repeated in her left thigh. “You’re protected for six months now!” the nurse exclaims. On that sunny March morning, in a small health center in Lobamba, a rural area of Eswatini, this 32-year-old sex worker has just become one of the first people in the world to receive lenacapavir, a drug that, administered twice a year, offers nearly 100% protection against HIV.
“I’m relieved. Several girls who work with me tested positive recently. I try to use condoms, but my clients don’t like it. Besides, they pay more without a condom,” explains Precious, who prefers to use a pseudonym in the interview.
This small country, located between South Africa and Mozambique, where UNAIDS estimates that 26% of its inhabitants — some 220,000 people — are living with HIV, the highest prevalence rate in the world, is one of the nine African states pioneering the distribution of lenacapavir. This drug opens a new chapter in prevention and could eliminate the virus as a public health threat by 2030.
“Eswatini, because of its small size and the progress it is already making in prevention, is a perfect place to start seeing results. And I think the world desperately needs a positive story related to HIV,” says Mark Edington, director of grant management at the Global Fund, the multilateral organization in charge of distributing these first doses.
Eswatini, because of its small size and the progress it is already making in prevention, is a perfect place to start seeing results. And I think the world desperately needs a positive story related to HIV
Mark Edington, Global Fund
Precious doesn’t know it, but the commercial price of the injection she just received exceeds $11,600, an amount that must be doubled to calculate the annual cost per person. This woman embodies “health equity” today, in the words of the Global Fund. Because it is the first time in the fight against AIDS that a new drug has reached the Global South at the same time as wealthier countries, and this is happening amid abrupt cuts in development aid that threaten the significant progress made against HIV.
A “solution,” especially for women
“Lenacapavir is a tremendous opportunity and will be a game-changer. That’s why the idea is that everyone who needs it in Eswatini can receive it,” says Sindy Matse, program manager for the AIDS Action Plan in the country, which still widely known internationally by its former name, Swaziland.
But for now, in this first phase of distribution, the drug’s doses are limited. In 2025, the Global Fund and the United States President’s Emergency Plan For AIDS Relief (PEPFAR) reached an agreement with the U.S. pharmaceutical company Gilead, the manufacturer of lenacapavir, to supply this pre-exposure prophylaxis (PrEP) to two million people in low- and middle-income countries until 2028. Generic versions are expected to arrive before then, in 2027, reducing the price to $40 per person per year. In total, nine countries, including Eswatini, Zambia, Kenya, Lesotho, and Zimbabwe, received these first doses of lenacapavir, and another 13 countries will be added to the list in the coming months.

Currently, more than 40 million people worldwide are living with HIV, 65% of them in Africa. Eighty-two percent of HIV-positive individuals on the continent are receiving treatment, compared to 45% a decade ago. “This injectable will be a turning point, a solution to the increase in positive cases among young people, especially girls,” Eswatini’s Minister of Health Mduduzi Matsebula told this newspaper. “I believe that by 2028 everyone in my country who needs lenacapavir will be able to receive it. And, little by little, the resources we no longer have to spend on treatment will be used for prevention,” he added.
— Do you think this drug could mean the end of AIDS as a public health problem by 2030?
— Yes, definitely.
Counted doses
Eswatini administered the first dose of lenacapavir on December 1, 2025, World AIDS Day, just months after its approval in the United States and Europe. To date, the country has received 4,200 units from the Global Fund, which will send another 1,800 in the coming weeks or months. Several thousand doses are also expected from the United States via PEPFAR, a program severely hampered by funding cuts.
“I knew I wanted the vaccine,” Precious repeats several times. Vaccine. That’s what the people waiting, seated on the reddish earth or under the shade of the generous trees at this clinic in the town of Lobamba, call lenacapavir. It’s one of 27 clinics administering the new drug in the country, where 59% of its 1.2 million inhabitants live in poverty. Most of the patients are young women who received information from healthcare workers or community educators.
“They sent us 50 doses, then 100, then 30. And every day more people arrive who have heard about this almost miraculous drug,” says Charles Mduli, the most senior nurse at this clinic, explaining that they had administered a total of 147 injections up to that day. “It’s the perfect treatment. It’s effective and completely discreet. Women come here who decide on their own to receive it and don’t have to explain themselves to anyone,” he adds.

Precious meets all the criteria to be considered at-risk, given her sex, age, and profession. She left her husband, the father of her two children, aged 13 and seven, two years ago after a beating that left her with a broken leg. “He almost killed me,” she explains. Since then, she and her children have been living with her mother. “I’ve been prostituting myself for over a year. I haven’t found a job, and I need to put food on the table, pay for school uniforms and supplies,” she explains. To survive, she needs about 4,000 lilangenis a month (around $230), and the math is clear in her mind. “A 15-minute encounter with a condom is 100 lilangenis, and without a condom, at least 150,” she explains.
It’s the perfect treatment. It’s effective and completely discreet. Women come here who decide on their own to receive it and don’t have to explain themselves to anyone
Charles Mduli, nurse in Eswatini
Precious had occasionally taken PrEP in the form of daily pills. But she found it difficult to be consistent, as is the case for many people who use it, because it’s a rather conspicuous method that draws questions or criticism from partners and family members, and because it requires more frequent visits to a health center.
“Most of the people who turn to lenacapavir in Eswatini and other countries had never taken any PrEP before. We are managing to attract people at risk, which is good news,” says Carmen Pérez Casas, strategic manager for HIV and pandemics at Unitaid, the international initiative working to improve access to treatment in low-resource countries.



Last September, Unitaid and the Gates Foundation announced separate agreements with Indian laboratories to make the generic version of lenacapavir available in 120 low- and middle-income countries starting in 2027. “But right now we’re running out of stock. Some centers have no doses left, others have enough for a few days. I hope the next shipment doesn’t take too long,” sighs Sindy Matse, from the national HIV program.
A visit to the central warehouse where medications are stored in Eswatini reveals that the shelf reserved for lenacapavir has very few boxes and plenty of space. Matse explains that the authorities have reserved 500 doses “just in case” for people who received the lenacapavir injection in December and are due for their second dose in May.
The impact of cuts
Authorities, health organizations, and experts agree that lenacapavir supplies will be limited in 2026, as Gilead, its sole manufacturer today, has already allocated all the doses it is capable of producing. Pérez Casas, from Unitaid, assures that the marketing of generic versions is progressing rapidly and they have already entered the World Health Organization’s (WHO) prequalification system.
“Only when generic drugs become available will we see a significant difference in infection rates. But if we don’t see any change by the end of 2027 or in 2028, then we’ll have to ask ourselves what’s going on,” says Edington of the Global Fund, the largest multilateral provider of funding for HIV/AIDS, tuberculosis, and malaria.
UNAIDS estimates that around two million people worldwide take some form of PrEP to protect themselves from HIV, the vast majority taking daily pills, but it estimates that to “drastically change the curve of new infections and move towards the end of AIDS by 2030” it would be necessary to reach 20 million people considered at risk.

In the corridors of the clinics in Eswatini visited by EL PAÍS, plaques commemorate the fact that these centers, dedicated to sexual health and prevention, received U.S. funding to open their doors. Sixty percent of Eswatini’s HIV response was funded through PEPFAR, and the impact of the abrupt funding cuts decreed by Donald Trump has been keenly felt.
The Minister of Health cites, for example, a reduced capacity for diagnostic testing, training of healthcare personnel, and maintenance of mobile units that traveled to remote areas to provide assistance to at-risk individuals who often do not visit health centers. “But the system has not collapsed, and the government is trying to address these shortfalls and expand its own capabilities so as not to always depend on external partners and donors,” he asserts. In December 2025, the U.S. and Eswatini signed a five-year memorandum of understanding on health matters, under which Washington plans to allocate up to $205 million to modernize public health data systems and disease surveillance technology, and to facilitate access to antiretroviral drugs for HIV.
According to UNAIDS, the impact of U.S. funding cuts could lead to, in the worst-case scenario, 6.6 million additional infections and 4.2 million more HIV-related deaths by 2029. Regarding prevention, figures published by the Clinton Health Access Initiative (CHAI) indicate that in 2025 the number of people who should have started oral PrEP was reduced by 37% compared to 2024 due to the cuts.
Men decide
Everyone in Eswatini knows someone living with HIV or who has died from AIDS-related complications. It’s a very real fear among young people in this country, which registers 4,000 new HIV cases annually, compared to more than 20,000 25 years ago.
“Lenacapavir is a milestone. Many people still don’t know this drug exists, and I think we need to be cautious until there is a greater supply,” says Nkululeko Dube, representative in Eswatini for the U.S.-based AIDS Healthcare Foundation (AHF). “But we mustn’t forget that lenacapavir protects against HIV/AIDS, but not against syphilis or pregnancy. People shouldn’t let their guard down,” urges Dube, speaking from the foundation’s LaMvelase clinic, the country’s largest medical center for HIV prevention and treatment.
The official still remembers the not-so-distant past when families in Eswatini had to sell their livestock and homes and were plunged into poverty in a futile attempt to save a son or brother suffering from AIDS. He also remembers the young people who died from pneumonia, meningitis, or other complications linked to the disease, and the people lying in the streets, exhausted and weakened by the lack of treatment. “It sounds like a movie, but that’s how it was.”
Another obstacle to prevention is the weight of a highly patriarchal society in a country where a significant portion of women depend on the will and finances of men, who also decide whether or not to use a condom during sex. “That’s just how things work here,” the women interviewed for this report repeatedly stated.
Sandra MKambule breaks those molds. She’s 24, runs a small beauty salon, and prides herself on being an independent woman. She received her first injection of lenacapavir in January because she doesn’t trust the men she has relationships with. “They don’t tell you the truth, and I want peace of mind,” she explains. “It was my decision, and nobody cares. It’s much more discreet than taking a pill every day. I think it’s going to change the lives of many young women like me,” she says, recalling that “some people can’t bear being sick,” like her 15-year-old niece, who found out she had contracted HIV and took her own life.
It was my decision, and nobody cares. It’s much more discreet than taking a pill every day. I think it’s going to change the lives of many young women like me
Sandra MKambule, businesswoman
“They don’t want to use condoms”
In Kayise Gama’s office at the Lyengo Clinic in Eswatini, there are three clear plastic containers filled with red and green beads, which she uses in her HIV prevention and treatment consultations. “The one with most green beads and a third red beads represents the person with HIV who comes to the clinic. The second one, with most red beads, represents that same person if they don’t receive treatment. The third one, where there are practically only green beads, represents the person after undergoing antiretroviral treatment,” she explains.
That day, Gama has two prostitutes in their early twenties before her, whom she must test for HIV before offering them lenacapavir. “I can’t protect myself because they don’t want to use condoms. And I don’t think much about myself because I have to bring money home,” sighs Princess, 27, who doesn’t want to give her real name. The young woman explains that she is responsible for her siblings, her two children, and her father. “I met an older man who paid me for sex, and I thought that was the life I was destined for,” she recalls, trying to hide her tears.
When she goes to the nurse’s office with her negative HIV test result, the girl must answer several questions before receiving the injection.
— Did you have unprotected sex in the last 72 hours?
— Yeah.
Princess won’t be able to receive lenacapavir that morning because the virus can take a few days to manifest even if the diagnostic test is negative. The nurse advises her to protect herself properly and return in a month. “You will, right?” she insists, seeing the young woman’s unconvinced expression.
“I was hoping to get my injection today, and I don’t know if I’ll be able to come back here again,” Princess says, disappointed.
Sign up for our weekly newsletter to get more English-language news coverage from EL PAÍS USA Edition